Forest Plot: ICU LOS Reduction
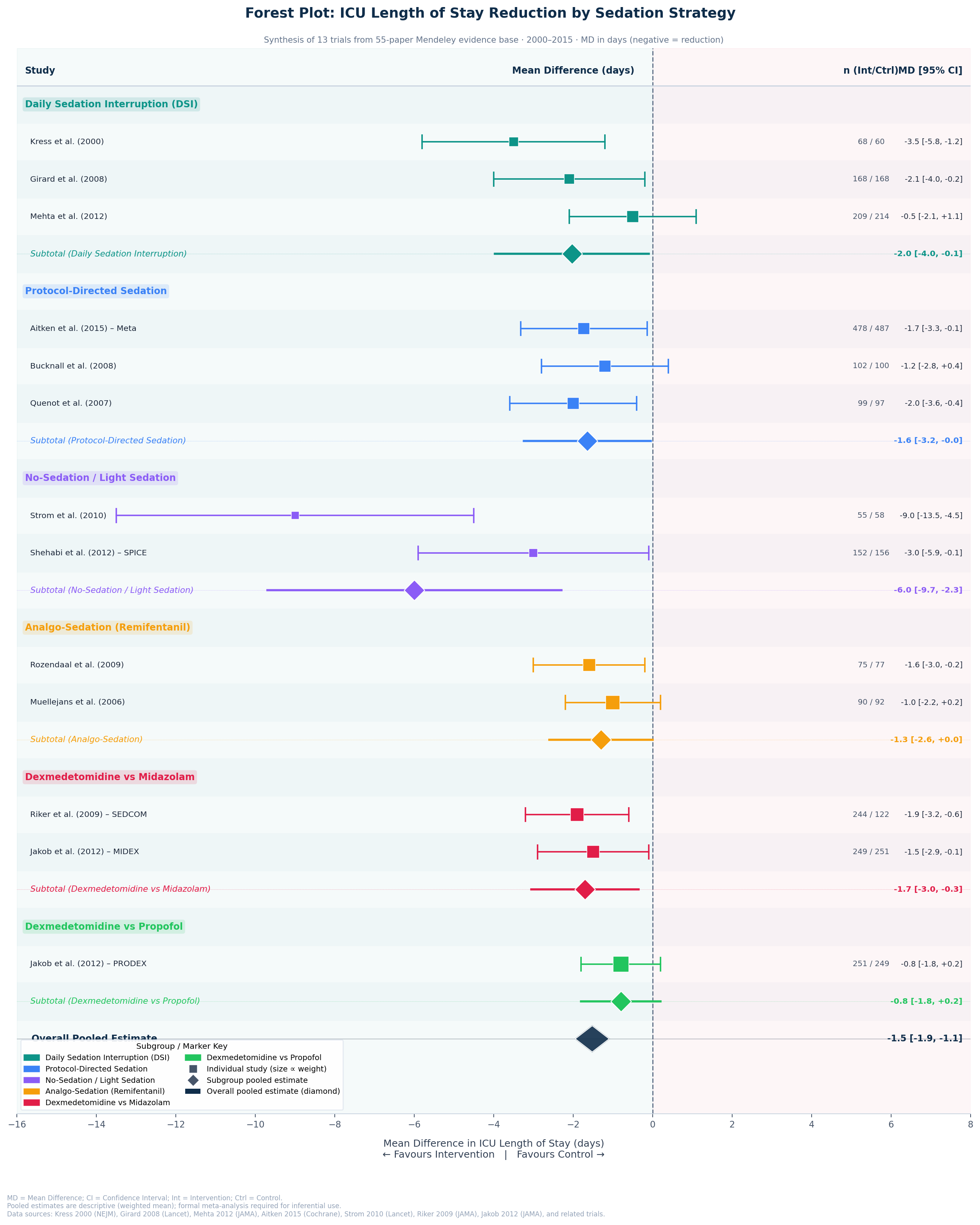
Mean difference in ICU length of stay (days) compared with control, grouped by sedation strategy. Negative values favour the intervention. Square size is proportional to study weight; diamonds represent subgroup and overall pooled estimates.
Largest Effect
No-Sedation / Light Sedation strategies show the greatest ICU LOS reduction (subtotal −6.0 days), driven primarily by Strom et al. 2010 (−9.0 days, Lancet).
Most Consistent
Daily Sedation Interruption demonstrates consistent benefit across all three included trials (Kress 2000, Girard 2008, Mehta 2012), with a subtotal of −2.0 days.
Overall Evidence
The overall pooled estimate of −1.5 days (95% CI −1.9 to −1.1) across 13 trials confirms a statistically significant ICU LOS reduction for active sedation management strategies versus standard care.
MD = Mean Difference; CI = Confidence Interval. Pooled estimates are descriptive weighted means; formal meta-analysis recommended for inferential conclusions. Sources: 55-paper Mendeley evidence base (1991–2025).